
The Method
Reflex Integration & Clinical Observations
It has become apparent through the thousands of assessments completed by Dr. Masgutova that as the number of non-integrated primary infant reflexes increase in an individual, the range and severity of motor, communication, and cognitive challenges and emotional and behavioral regulation issues correspondingly increase. In 2004, Dr. Masgutova and her team tracked primary infant reflex assessment results for a population of 850 children, ages 1-12. The children and their conditions were classified according to the predominant diagnoses provided by their parents. From this work emerged the following general non-integrated reflex profiles for each characterized condition:
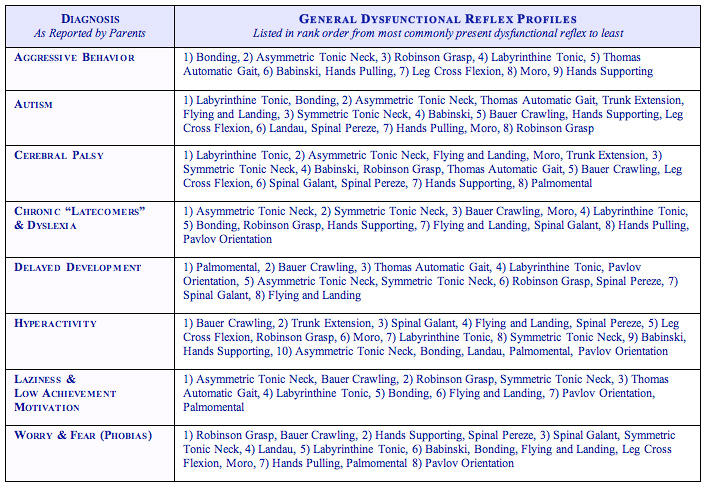
It is important to note that these are general, non-integrated reflexprofiles and are shared here to provide perspective regarding the primary infant motor reflexes that might not be integrated for individuals diagnosed with these conditions. Please remember that each individual is unique in their strengths and challenges and, therefore, should be assessed by a qualified MNRI trained resource to determine the actual integration status of primary reflex patterns for each individual.
Reflex integration can change lives. The verbally delayed child can begin to form intelligible sounds, words and/or simple sentences. Individuals with hypertonic rigidity can begin to relax clenched fists, rigid arms and/or legs. The disorganized may begin to move toward self-organization, the dysgraphic to write legibly, the sensory defensive to tolerate sounds, sights and/or touch opening up positive interaction with the world, shifting from an inner state of constant fear, distrust and concern to calm, wonder and joy. The prognosis and outcome for those accessing MNRI Method techniques will vary based on the:
- Underlying cause of the condition -- Congenital disorders, trauma, chronic prolong or intermittent stress, or disease.
- Which, how many, and to what extent the underlying neural, sensory and motor systems supporting reflex function are challenged.
- Number and combination of primary infant reflexes are impacted as well as the developmental maturity of each impacted reflex.
- Developmental time frame within which reflex integration work is completed -- before, during, or after the typical maturation and integration time period, and the
- Rigor with which reflex integration work is completed.
Regardless of the magnitude, complexity, or apparent level of debilitation an individual faces, it is important to understand that dysfunctional or more deeply pathological primary infant motor reflexes, when addressed with the right combination of integration techniques, can lead to improved or even restored function. While the magnitude of the underlying neurosensorimotor challenges may limit the degree of restoration when addressed with the right combination of integration techniques, almost every individual may experience some level of functional improvement – moving them a step closer to reaching their unique potential. The first step to beginning this process is simply learning about the impact integrated primary infant reflexes can have on improved function. The next steps include identification of dysfunctional or pathological reflexes and figuring out the best way to begin the integration process. To learn more about beginning the integration process refer to our website section regarding treatment options. The earlier underlying neurosensorimotor challenges can be identified, the easier it will be to minimize or even eliminate the impact dysfunctional or pathological reflexes can have on overall maturation and development.